The Social Innovation
Founded in 2012, Healthy Entrepreneurs set out to solve one of global health's most persistent failures: the inability of our systems to deliver affordable, quality primary healthcare to remote and rural communities across Sub-Saharan Africa.
Their answer is the Community Health Engagement Model (CHEM) — a micro-franchise that activates existing infrastructure rather than building a parallel system. At its center is the Community Health Worker (CHW): predominantly women living below the poverty line, equipped, trained, coached, and supplied by Healthy Entrepreneurs to become Community Health Entrepreneurs — professional, income-generating care providers embedded in their own villages.
Community Health Entrepreneurs (CHE) offer door-to-door services covering prevention, point-of-care diagnostics (malaria, blood pressure, HIV, pregnancy), essential health commodities, and chronic disease management — complementing, not replacing, the national community health program. Products are offered at 10–15% below market rates; Community Health Entrepreneurs earn a 35% gross margin. This is not charity — it is a livelihood. A Virtual Clinic and eDispensing system connects them in real time with licensed professionals for remote consultations and ePrescriptions, bringing care to the village without requiring patients to travel. And a layered financial inclusion model — credit, income insurance, and an emergency fund — makes all of this accessible from an initial investment of just $20.
The results speak for themselves. Community Health Entrepreneur income increases by up to 70%, dropout rates after seven years remain below 10%, and community out-of-pocket health expenditure drops from 15% to 6–8% of annual household income — below the Universal Health Coverage benchmark of 10%.
Today, Healthy Entrepreneurs operates across Uganda, Tanzania, Kenya, DRC, Nigeria and Burkina Faso with over 20,000 Community Health Entrepreneurs serving an estimated 13 million people, supported by 115 staff — 97% national.
Magnitude of the Problem, and its Root Causes
More than 600 million people in remote and rural villages across Sub-Saharan Africa lack reliable access to quality primary healthcare. A health centre can be 3–8 hours away. Private pharmacies charge prices rural families cannot afford. And 30–60% of medicines available in informal markets are falsified or counterfeit.
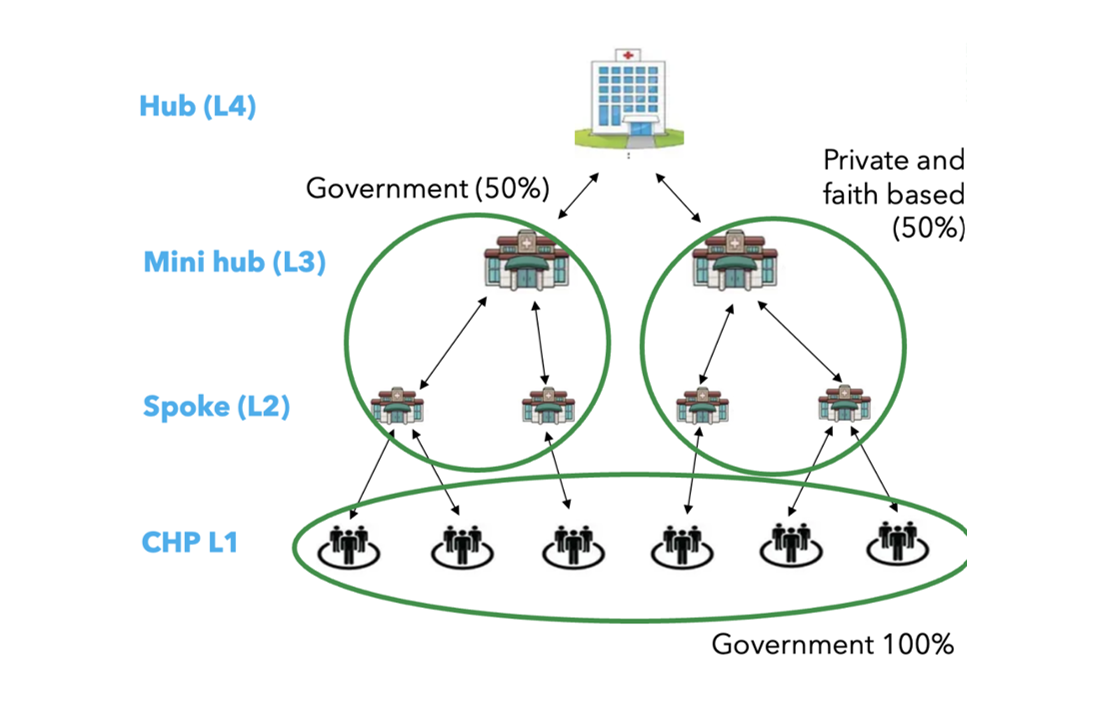
A critical but overlooked dimension of this crisis is structural: at the community level (L1), healthcare is 100% managed by government, with no formal role for private sector actors. Instead, all social investment and innovation in health have concentrated at L2, L3, and L4 — the facility and hospital tiers — where the private sector does have a foothold.
"You will not see any other social venture actually trying to improve service provision using private sector tools where they're competing or complementing government. In our case, we are a unique single unicorn that actually operates at this lower level, complementing the government or national system."
Community health workers exist as the theoretical first line of care at L1. But they are underfunded, undersupplied, and are underpaid making it very difficult for them to sustain their role. Families, meanwhile, spend approximately 15% of their annual household budget on healthcare, with more than 55% of that cost going to transport rather than treatment.
During their participation in the Globalizer co-created by Ashoka and Philips Foundation in 2016, the Healthy Entrepreneurs team identified the following key root causes contributing to the magnitude of the problem:
- No functioning market at the last mile: people who need care cannot access it due to cost, distance, and structural invisibility
- An unsupported CHW workforce: community health workers lack financial incentives, supplies, and professional infrastructure to perform effectively or remain in their roles
- Fragmented and unreliable supply chains: medicines and health products do not reliably reach remote communities, and where they do, quality is often compromised
- Weak regulatory frameworks for community-level innovation
Based on their systems change analysis, the Healthy Entrepreneurs team made it a mission to transform the role of community health worker from under-resourced volunteer into professional, income-generating care provider — and to do so at scale: six million strong across Sub-Saharan Africa, creating a self-sustaining market for primary healthcare at the last mile that governments can integrate and scale nationally.
"There is a moment every innovator faces: is it worth it? The Globalizer gave me the framework to understand that a journey like this takes at least 20 years — and we are only halfway. What I found there was not just strategy. It was the recognition that thinking 15 to 20 years ahead and working backwards is not crazy. It is exactly what systems change requires."
Strategy to Catalyze a Network of Changemakers towards the Targeted Mission
Healthy Entrepreneurs’ strategy centres on building a financially sustainable micro-franchise model that governments, research institutions, investors, and implementing partners can adopt, integrate into national health systems, and replicate at scale — making quality last-mile healthcare the norm, not the exception.
The journey involves three phases: discovery, distribution at mass scale, and ultimately democratisation — the full embedding of the model into national systems. They are currently in the second phase, having spent a decade proving the model works and now building the infrastructure to take it to 100,000 Community Health Entrepreneurs across 5 countries.
Some of the tactics deployed towards the mission as part of the strategy include:
1) Collaborating with Research Institutions to Build Evidence on the Value of Involving & Equipping Community Health Workers to Influence Adoption
To drive adoption at government and policy level, Healthy Entrepreneurs has invested systematically in rigorous, independent evaluation of the Community Health Engagement Model's impact.
A growing body of evidence backs the model: 6 publications since 2019 — co-produced with partners including Oxford, LSHTM, Vrije Universiteit Amsterdam, Makerere University, and Uganda's Ministry of Health — document impact on healthcare access, gender equity, and system resilience.
Key findings across this body of evidence include:
- 62% reduction in out-of-pocket health expenditure per beneficiary,
- 40 hours per year saved in travel time,
- 100% increase in use of modern contraceptives, and
- 30% reduction in stroke risk for chronic disease patients managed through the Virtual Clinic.
- Independent evaluation by 60 Decibels (2024) found that 96% of beneficiaries report improved access to healthcare and 72% accessed a Community Health Entrepreneur for the first time.
The publications are consolidated here.
This evidence base supports Healthy Entrepreneurs' recognition by the World Health Organization as a Top 10 Innovator for Primary Health Care — a designation that has transformed conversations with previously reluctant global institutions.
"10 years ago, UNICEF would not have been willing to talk with me. Nowadays, given the impact of our model, they are interested in working with us to see how this model can actually help them achieve their objectives. It requires persistence, it requires continuity, and it requires just continuing to showcase. I haven't found the golden formula about how to do so yet."
2) Co-creating with Ministries of Health to Integrate and Institutionalise the Model within National Health Systems
From the outset, Healthy Entrepreneurs has designed the Community Health Engagement Model in formal partnership with governments — not in parallel to them. In every country of operation, the model is co-designed with the Ministry of Health and formalised in a Memorandum of Understanding (MoU) that defines the portfolio of products and services, the distinction between free government-supplied commodities and subsidised the Community Health Engagement Model products, roles and responsibilities at every tier of the health system, and data reporting and ownership arrangements.
This approach reflects a hard-won shift in the relationship between Healthy Entrepreneurs and the ministries of health. For years, Joost describes, governments were resistant and conversations were defensive.
Today, the dynamic has changed fundamentally:
- A landmark indicator of this integration came when Tanzania's Ministry of Health formally embedded the Community Health Entrepreneurship Module (CHEM) as Module 9 in its national Community Health Worker training curriculum — placing it alongside modules on maternal health and communicable diseases as a standard component of national workforce development.
- In Kenya, the Community Health Engagement Model activities are now registered in the national electronic Community Health Information System (eCHIS), and treatments provided by Community Health Entrepreneurs s are reimbursed through the Social Health Authority (SHA) national insurance scheme.
- MoUs are currently active in Burkina Faso, DRC, Kenya, Nigeria, Tanzania, and Uganda, with an Ethiopia working group in progress.
"The conversation nowadays with government is very different from 10 years ago. There's no more need to be defensive, no more need to explain the model — it is now more the conversation of how to start working together."
3) Leveraging AI & Tech Advances to Consult CHEs and Sustain Quality as the Network Scales
As the Community Health Engagement Model scales, Healthy Entrepreneurs is investing in artificial intelligence and machine learning to sustain quality at a level manual system cannot maintain.
The staff isn't able to go through all the data, and the team is now counting on AI to do so, and take recommendations on how to actually grow the performance of health workers. Three priority use cases are in development:
- Household health profiling: a predictive model scoring households by health risk — drawing on family composition, pregnancy status, NCD screening data, and child growth monitoring — to enable proactive, targeted interventions
- Intelligent inventory management: AI-driven forecasting of optimal stock levels per CHE, incorporating historical sales data, seasonal disease patterns, and regional health data
- Field decision support: a lightweight mobile AI assistant guiding Community Health Entrepreneurs through consultations in real time — based on local treatment protocols and patient data
For the engagement team managing 20,000+ Community Health Entrepreneurs, machine learning will also enable dynamic performance profiling and automated, personalised coaching scripts generated from each Community Health Entrepreneur’s household outreach data.
4) Collaborating with Impact Investors and Strategic Partners to Fund and Replicate the Model at Scale
To move from proof of concept to national-scale infrastructure, Healthy Entrepreneurs has built a hybrid funding architecture combining impact equity, concessional debt, and grant funding.
Equity has been invested by the Philips Impact Investment Fund and Madiro Impact (Canada) and working capital for the supply chain is financed by the Dutch Good Growth Fund (DGGF). Strategic implementing partners include Grand Challenges Canada, the Dutch Ministry of Foreign Affairs, Amref Health Africa, CARE USA, WHO, Philips, and Bayer.
"Philips invested as a result of the Globalizer. They committed to continuing if we bring in larger investments — and they were clear: they care more about the model being scaled and replicated globally than getting their money back. They are very impact driven."

The model is projected to reach break-even in 2028. With a EUR 45 million funding need for 2026–2030, Healthy Entrepreneurs aims to expand to 100,000 Community Health Entrepreneurs across 5–7 countries — reaching 100 million people by 2030 and 250,000 Community Health Entrepreneurs by 2035, realising an estimated $6 billion in health savings for rural families across Sub-Saharan Africa. The ambition is a system that doesn't just scale — it gets smarter as it grows.

For more than 40 years, Ashoka has built and nurtured a network of 4000+ leading social entrepreneurs in the world. Read more about the Ashoka Fellowship here.
- 2016,
The Globalizer strategy accelerator supports social entrepreneurs gain clarity on systemic root causes of social and environmental problems and the importance of engaging more changemakers as part of the solutions. It enables them to design effective collaborative systems change strategies (based on respect to all humans and nature).
Refined since 2010, the accelerator is a structured collective thinking and experimenting process between social entrepreneurs, systems thought partners from Ashoka and selected leaders from business and the social sector.
Participated with support from
Elements of the Collaborative Systems Change Strategy
Hover/Click on things to dive deepType of Root Cause identified as a Leverage Point for Systems Change (Donella Meadows)
The first element of crafting a collaborative systems change strategy to address a problem is to define the problem and identify the most strategic change needed to address the root cause(s) of the problem. That becomes the targeted Systems Change Goal or the Mission.
To identify it, analyze the root causes—barriers, factors, dynamics, points or conditions driving the problem—and determine which offers the greatest leverage for change.
According to the FSG, leverage points include:
- Policies
- Practices
- Resource Flows
- Relationships & Roles
- Power Dynamics
- Mental Models
These "leverage points" are derived from the work of Donella Meadows, the pioneer in the field of systems thinking who articulated and conceptualized "Leverage Points: Places to Intervene in a System to Create Effective Change".
Explore Case Studies of different types of "Systems Change Goal(s)" in our Library.
Endgame / Pathway applied towards Activating a Network of Changemakers towards the targeted Systems Change
The second element of crafting a collaborative systems change strategy includes determining how to achieve the systems change goal.
This means choosing a strategy suited to the system’s context. The strategy could be to:
- Work with government
- Create a new field/market
- Build a competitive advantage
- Shift societal narratives
The items on the list are neither mutually exclusive, nor collectively exhaustive.
You can read more about the types of systems change strategies/pathways/endgames/stories we have come across in this article by Odin Muehlenbein.
Explore Case Studies on different "Types of Strategy" in our Library.
Types of stakeholders activated as changemakers towards the systems change
The third element of crafting a collaborative systems change strategy includes identifying the critical stakeholders to activate as partners- those who influence an exponential number of people in the context of the system.
Irrespective of the type of strategy, systemic change always requires activation of a network of stakeholders for different tactics towards the mission.
Typical stakeholder groups for systemic change include:
- government agencies
- universities (e.g. education schools for the empathy paradigm, public health and med schools for the health paradigm, etc.)
- publishers (e.g. education publishers for empathy, medical journals for health, etc.)
- informal & formal communities / unions (e.g. AARP for longevity, teachers' unions for empathy, families, etc.)
- media companies
- industry-specific companies / organizations (e.g. tech companies and financial institutions for the technology paradigm, insurance and healthcare companies for longevity, relevant civil society organizations etc.).
Explore Case Studies on different "Types of Partners Engaged" in our Library.
The depths of engagements in play for the different stakeholders (CoCreative)
The fourth and final element of crafting a collaborative systems change strategy includes reflecting on what depth to engage with each stakeholder.
Activating a broad network is essential, but so is clarifying their role: Are they simply informed, consulted, or co-creating the strategy?
CoCreative's Five Levels of Engagement Framework guides how one may engage with each stakeholder. Are you:
- co-creating?
- collaborating?
- involving?
- consulting?
- informing?
Explore Case Studies on different "Levels of Stakeholder Engagement" in our Library.
Their work contributes towards



The 2030 Agenda for Sustainable Development, adopted by all United Nations Member States in 2015, provides a shared blueprint for peace and prosperity for people and the planet, now and into the future. At its heart are the 17 Sustainable Development Goals (SDGs), which are an urgent call for action by all countries - developed and developing - in a global partnership.
Explore Case Studies on strategies contributing to addressing different "SDGs" in our Library.
The root causes of global socio-ecological unsustainability their work is addressing (FSSD)
According to the Framework for Strategic Sustainable Development (FSSD) co-created by Ashoka Fellow Dr. Karl-Henrik Robèrt and Dr. Göran Broman and Dr. Merlina Missimer of the Blekinge Institute of Technology, Sweden, there are 8 root causes of all socio-ecological unsustainability problems (also referred to as Sustainability Principles):
- extraction from Earth's crust
- chemical pollution
- physical destruction
- barriers to health
- barriers to competence
- barriers to influence/participation
- barriers to impartiality
- barriers to meaning-making
To get a deeper feel, here are videos on the ecological and social sustainability principles.
You can see case studies of changemakers contributing to addressing different root causes ("Sustainability Principles") in our Library.



